BLOG
“This is an online e log book to discuss our patient’s de- identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patient’s clinical problems with collective current best evidence based inputs. This e-log book reflects my patient centered online portfolio and your valuable inputs on the comments is welcome.”







A 45 year old male a daily wage labourer by occupation ,resident of nalgonda came to the opd
CHIEF COMPLAINT
Dialysis(MHD)
History of presenting illness
The patient was apparently asymptomatic 2 years back when he had experienced weakness in right lower limb, upper limb and numbness in lips which initially stayed for half an hour.
Upon walking it relived but again presented the next morning,so was admitted to a hospital where it was considered as cva revealed that he had high creatine levels and was treated
He was also diagnosed as denovo hypertension
He used tablet for three to four months in lieu of high creatine levels and discontinued after improvement of symptoms
2 months back he went to a hospital in nalgonda with complaints of shortness of breath, and edema where he was deemed as chronic kidney disease and was required to do dialysis
He was referred to a hospital in hyderabad where he had dialysis 5 times
Then 1 month ago He came to our hospital for the dialysis and complaints of shortness of breath and pedal edema pitting type till knee 1 month
He had 10 times dialysis
Now he has complaints of shortness of breath and pedal edema pitting type till knee
And came for maintenance dialysis
He had dialysis till date 17
History of past illness
No history of Diabetes mellitus
Thyroid disease
Bronchial Asthma
Tuberculosis
He is a hypertensive since 2 yrs with inconsistent treatment
Stroke 2 years back?
PERSONAL HISTORY
Married
Appetite-Decreased
non vegetarian
Bowels- adequate movement
Micturition- no complaints of decreased or burning micturation
Addictions- occasional alcohol consumption
smoking but stopped 2 months back(1-2 packs)back
Daily routine before 2 years
5:00 woke up
6-7:00 had breakfast
9:30 went to work
1:00 lunch
8:00 comes back and watches tv
8-9:00 dinner
9:30 sleep
Daily routine after pain
Stopped going to work
Still wakes up at 5 but then
Eats and sleeps
Sometimes watches tv
Dietary history
Breakfast- Dosa
Lunch rice and curry
Dinner rice and curry
Occasionally drinks a glass of milk
FAMILY HISTORY
No significance
General examination
The patient is conscious coherent and cooperative
Patient is thin with signs of muscle wasting
Pallor is there
NO Icterus
NO Cyanosis
NO Koilonychia
NO Lymphadenopathy
PITTING TYPE OF EDEMA
VITALS
Afebrile
BP :140/90 mmHg
Pulse rate : 99
Respiratory rate : 18
SPO2 at room air :99%
SYSTEMIC EXAMINATION
CVS
NO Thrills
S1 and S2 heard +
NO murmurs
RESPIRATORY SYSTEM
Position of trachea: central
NO wheeze
NO dyspnoea
ABDOMEN
Shape : Scaphoid
NO Tenderness
No palpable mass, fluid , bruits
CNS
Higher functions intact
Patient is conscious, coherent,and co operative
Patient is oriented to time place person
No delay in response
Crainal nerve intact
Examination of motor system
Tone normal
Power of muscle normal
Coordination of movement normal
Provisional diagnosis
Chronic kidney disease on maintenance dialysis
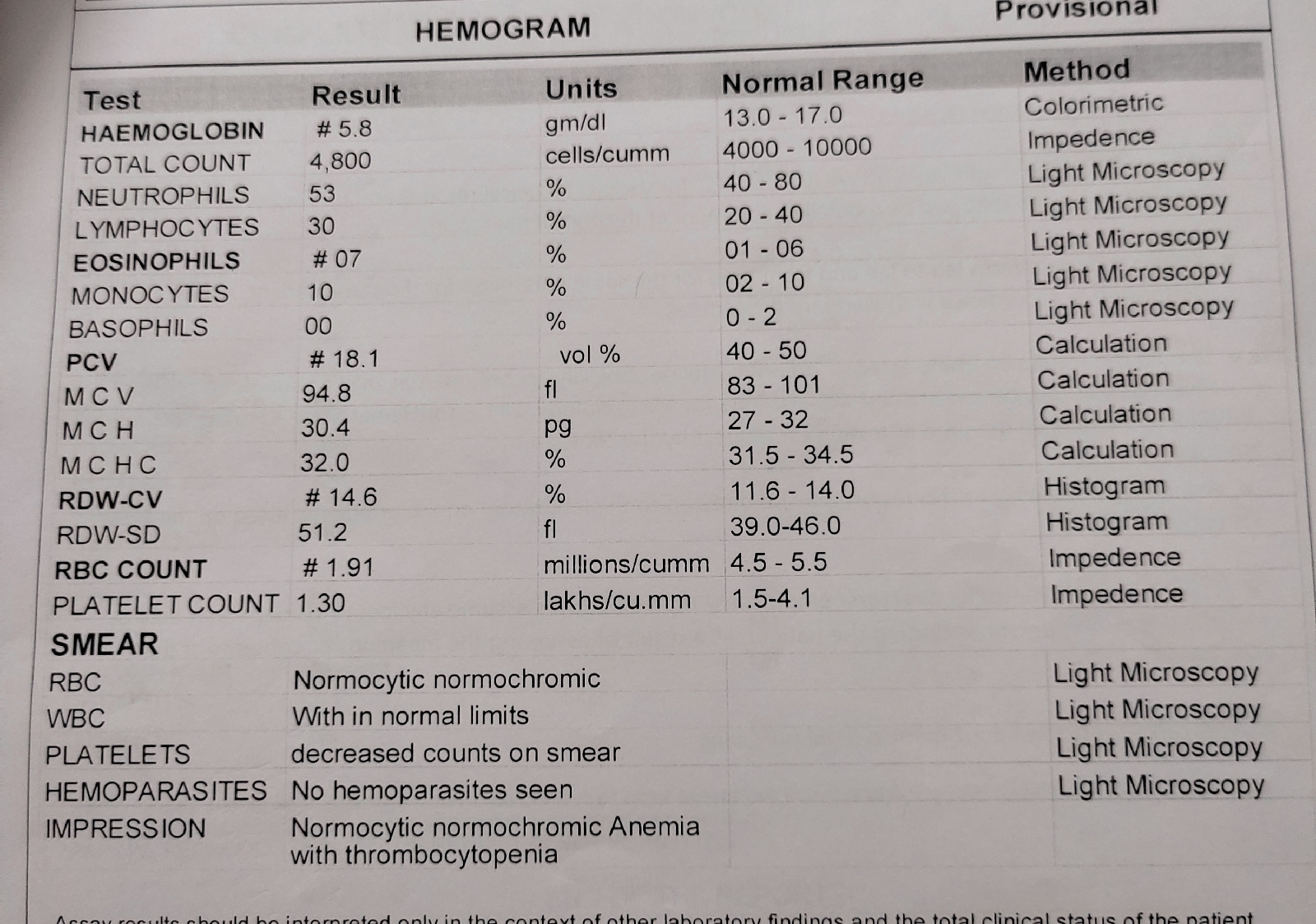
INVESTIGATIONS
Treatment plan
Day 1
S :-
O:-
Pt is conscious, coherent cooperative
Bp:-140/70
Pr:-92 bpm
Cvs:-s1s2+
R/s:-BLAE +
P/A:- soft , non tender spleenomegaly
CNS:- NAD
A:-
P:-
Vital monitoring
Temperature monitoring


Comments
Post a Comment